


Basic Brain Imagingfocus on stroke
Adam Guttentag M.D.
All photos retain the copyrights of their original authors
© 2005 Adam Guttentag, MD
Stroke
Acute change in neurological status.
Symptoms persist longer than 24 hours.
Resolution in less than 24 hours = TIA
Ischemia 80%
Embolic
Thrombotic
Hemorrhage 20%
Stroke = “Brain Attack”
Rapid clinical and imaging evaluation.
“Stroke team” needed
Thrombolytic therapy for appropriate patients
<3 hours from onset of Sx
No contraindications to tPA (long list)
Involvement of large area of brain acontraindication
Risk of hemorrhage from tPA
Assessed by imaging and clinical evaluation
CT usually negative in the first few hours
Acute strokeInitial imaging
CT without IV contrast
Rapid
Reliable to exclude hemorrhage
High sensitivity for acute blood
Acute blood appears bright on CT relative tobrain tissue.
IV contrast only if suspicion of anotheretiology, e.g. tumor or AVM
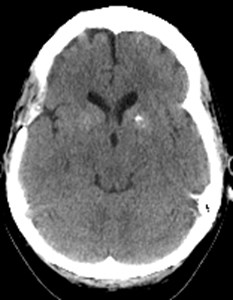
Normal 40 year old
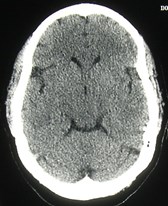
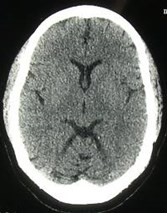
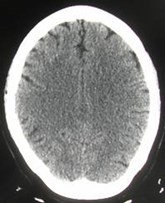

Normal 65 year old
Ischemic StrokeCT
1st 6 hours:
60% normal
Vague hypodensity in ischemic area.
Insular ribbon sign
Sulcal effacement from slight swelling
Loss of grey/white interface
12-24 hours
More apparent hypodensity
Minimal mass effect
Ischemic StrokeCT
After 24 hours
Well circumscribed hypodensity
3-5 days
Peak mass effect
Mass effect gone by 2-4 weeks
Long term
Ex vacuo dilatation of ventricles
Encephalomalacia in infarcted area
Acute right sided weakness


24 hours later





Insular ribbon sign

Acute MCA Infarct - Insular ribbon signCT
Dense MCA signCT
Thrombus in vessel is hyperdenserelative to flowing blood

Initial scan

7 hours later
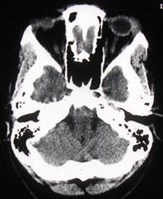
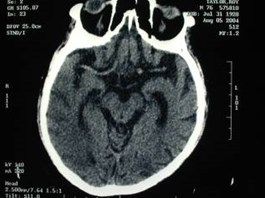
Basilar artery thrombusCT
Equivalent to dense MCA sign


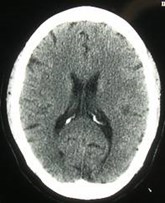
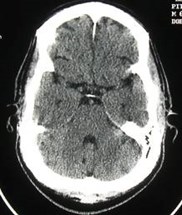
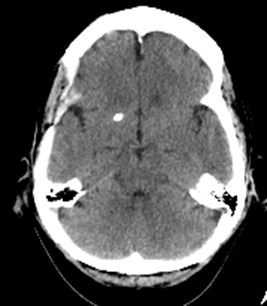
Acute left hemiplegia
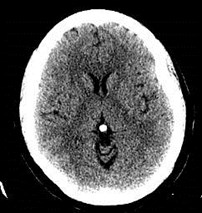
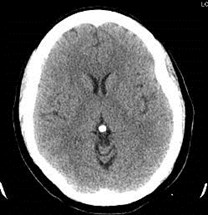
One month earlier
Newdecreaseddensity inright basalganglia
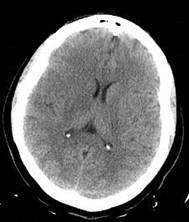
Acute Right MCA infarctCT

Minimal mass effect
Well circumscribedinfarct
Cytotoxic edemapattern
Differentiating cytotoxic fromvasogenic edema
Cytotoxic
Grey and white matter
Wedge shape
Infarct
Vasogenic
Almost exclusively inwhite matter tracts
Finger-like projections
Infection, XRT, tumor

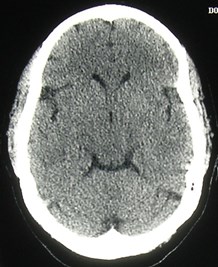
Diffuse cerebral edema fromhanging

Poor differentiation of gray from white matter
No sulci visible
normal
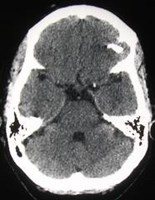
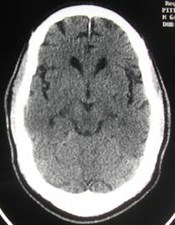
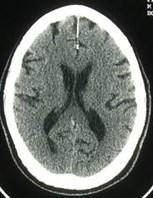
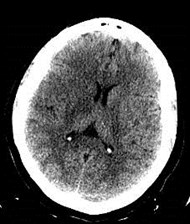
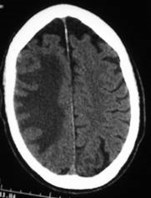
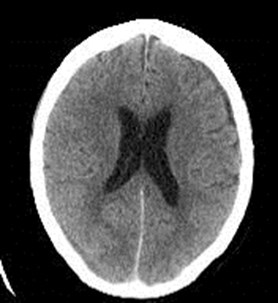
Acute ΔMS: New stroke?
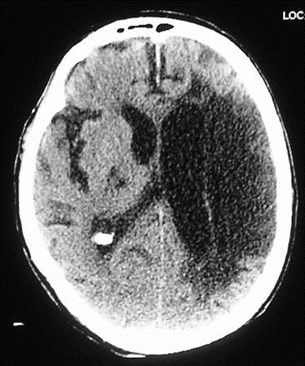
Very low density infarcted brain
Dilated ventricle adjacent to infarct
Oldstroke
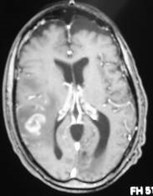
Ischemic StrokeCT
Contrast enhancement
Not usually indicated unless there’ssuspicion of a different process
Enhancement in infarcted area begins afterabout three days
Enhancement more than 6-8 weeks afterictus suggests another etiology
New role:
“Perfusion” scans of brain with rapid IV contrastinfusion.
Ischemic StrokeCT– limitations
Low sensitivity for acute ischemic infarct
Decision to use thrombolytic based onabsence of CT findings
Potential use of thrombolytic in patients withoutthrombotic or embolic infarct
Arterial dissection
Postictal state
Infection or tumor
Up to 40% of acute strokes are not from causesamenable to thrombolysis
20% without defect seen on angiogram
10-20% from small vessel disease or arterial dissection
Acute stroke:Initial imaging
MRI
Diffusion weighted images take only ~2minutes
highly sensitive for acute ischemia
Contraindications
Pacer, AICD, aneurysm clip, etc
Full imaging takes ~30 minutes
Special MR compatible life support andmonitoring equipment needed
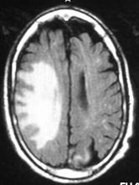
Ischemic StrokeMRI
Glossary - types of pulse sequences
T1WI- images where signal depends on T1 oftissues
T2WI- images where signal depends on T2 oftissues
FLAIR = FLuid Attenuated Inversion Recovery
Images with pathology bright and CSF dark
DWI = Diffusion Weighted Imaging
Fast acquisition where signal depends on ability of waterto diffuse in all directions
Ischemic StrokeMRI
Acute stroke appears as
Normal to low signal on T1WI
High signal on T2WI
High signal on FLAIR
High signal on DWI
FLAIR and DWI most sensitive
Ischemic StrokeMRI
Abnormal area becomes bright on DWIwithin 30 minutes of onset of ischemia
High signal visible on T2WI in about 8hours
T1WI image becomes abnormal after~16 hours
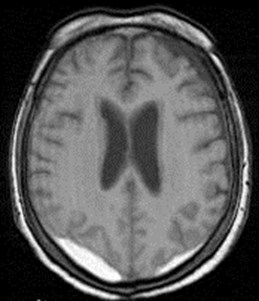
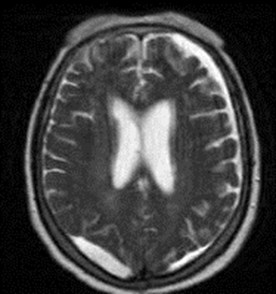
Ischemic StrokeMRI
Infarcted area remains bright on T2WIforever.
As encephalomalacia occurs, infarctbecomes progressively darker on T1WIuntil it matches signal of CSF
Ischemic StrokeDiffusion Weighted Imaging
Requires high field magnet with rapidgradients
In ischemic tissue, diffusion of watermolecules in 3 dimensions is restricted
Magically, these areas appear as brightareas on DWI
Ask a physicist how it works…
Ischemic StrokeDiffusion Weighted Imaging
Area of ischemia visible within 30minutes
10-14 days later, diffusion is “normal”
Brain becomes isodense
Late, with encephalomalacia, area showslow signal
T2WI becomes progressively brighter withrespect to DWI as infarct ages
crossover at about 3-7 days
Ischemic StrokeDiffusion Weighted Imaging
Signalintensity
Time
stroke
DWI
T2WI
3-7 days
Ischemic StrokeDiffusion Weighted Imaging
Super-sensitive
Not super-specific
False positives:
Hemorrhage
MS
Abscess
Lymphoma and other tumors
In uncertain situations, repeat in 2 weeks
Infarct should normalize on DWI
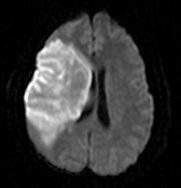
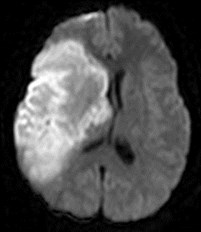
Hyperacute Left MCA infarctMRI

T2WI

DWI

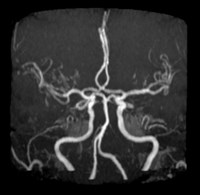
MRA
L MCA occluded
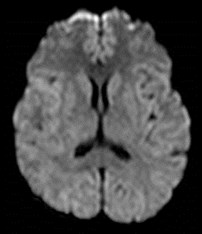
Subacute InfarctMRI
Dark on T1WI, bright on T2WI and FLAIR, very bright on DWI
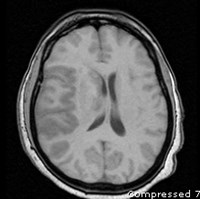
T1WI
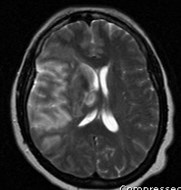
T2WI
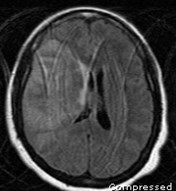
FLAIR
DWI
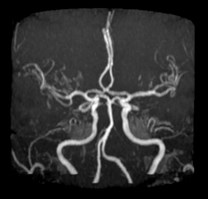
One month earlier
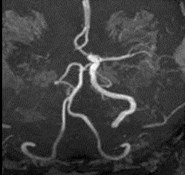
Absent R ICA and MCA
Acute R ICA occlusion
MRA in acute stroke?
Good for seeing larger intracerebral vesselsonly.
Not generally useful unless intervention isplanned very early.
In most strokes, treatment is not usuallyaffected by identification of an occludedvessel.
Ask your neurologist if the information isuseful.
Not all ischemic damage is due toacute thrombosis or embolism:
Vasculopathies:
Diabetic
Hypertensive
Giant cell (temporal) arteritis
Takayasu’s arteritis
PAN
Sarcoid
Collagen vascular diseasesesp. SLE
Wegener’s granulomatosis
drugs
Larger vesseldisease
Moyamoya
Fibromuscular dysplasia
Infectious disease
Syphilis
TB
Herpes
Nonvascular
Global hypoxia
CO poisoning
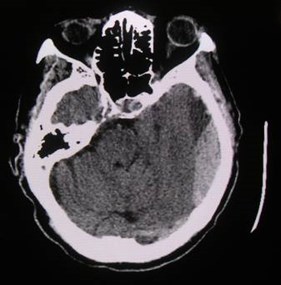
Hemorrhagic strokeCT
CT best for finding acute bleeding
Normal white matter = 30-34 HU
Normal grey matter = 37-41 HU
Attenuation of blood depends onhemoglobin conc.
Blood with Hct of 45% = 56 HU
Acutely extravasated blood will be denser thanbrain and easily visible
Clotted blood, e.g. subdural hematoma, will beeven denser.
By the way, what are HU?
Hounsfield Units
Measure of CT density
H20 = 0 HU

Sir GeoffreyHounsfield
Intracranial hemorrhage -possible locations
Intraparenchymal
Intraventricular
Subarachnoid
Subdural / epidural



Hemorrhagic strokeCT
Acute bleed in anemic patient will beharder to detect.
With Hct <30%, nonclotted blood may beisodense with brain.
Highest clot density at about 72 hrs afterbleed
High density disappears after severalweeks
Intraparenchymal Bleedinglocation, location, location…
Hypertensive bleed - most common (80%)
Basal ganglia
Thalamus
Pons
Cerebellum

Don’t be fooled:
Normal variant: calcification in the basal ganglia(usually symmetric)
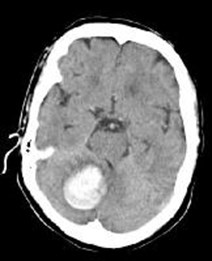
Intraparenchymal Bleeding
Atypical locations like cerebral hemispheres
AVM
Aneurysm
Berry and mycotic
Trauma
Amyloid angiopathy
Tumor
Vascular mets, primary tumors
Vasculitis, cocaine, amphetamine, bleeding diathesis,anticoagulation, etc
Intraparenchymal bleedCT — natural history
Accompanied by vasogenic edema, somemass effect
Consider enhanced scan for mass effect out ofproportion to size of hematoma
Possibility of underlying tumor
Later, some peripheral enhancement may beseen
Confusion with other etiologies
Much later, thin slit of hypodensity is seen atsite of bleed.
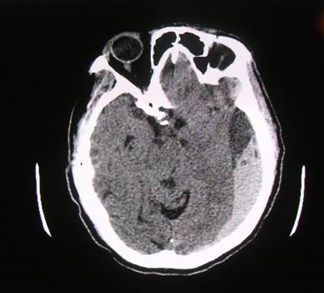
Berry aneurysm
Trauma
Subarachnoid hemorrhage

Subarachnoid hemorrhageBerry aneurysm
80-90% of subarachnoid bleeds
Prevalence 1-5%?
Familial vs. sporadic
Adult polycystic kidney disease (10% of pts)
Marfan’s, Ehlers-Danlos
Fibromuscular dysplasia
Multiple in 15-20%

Subarachnoid bleedingBerry aneurysm
Mortality 10-15%
Often re-bleed in first day
50% will re-bleed within 6 months
Angiogram and treatment early
Before onset of arterial spasm leading to infarction
MRA or CTA?
Rapid (2-3 minutes)
No need for specialized call personnel
Endovascular therapy vs. surgery
Subdural and Epidural Hematoma
Usually traumatic in origin
Subdural
Venous bleed
Low pressure
Slow growth
Epidural
Arterial bleed
High pressure
Rapid growth
Both may be life-threatening from mass effectand herniation
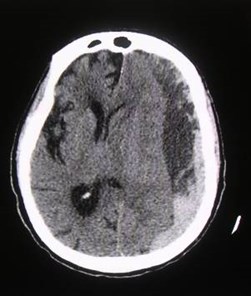
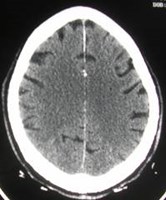
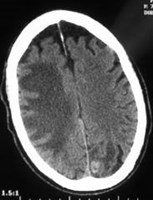
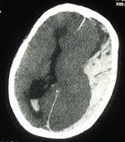
Acute subdural hematomaCT
Midline shift
Basal cisterneffaced=earlyherniation
Intraventricular Hemorrhage
Trauma
Hypertension
Aneurysm

Hemorrhagic strokeMRI
Signal from blood depends on pulsesequence, age of clot
Hemoglobin contains iron
Strong paramagnetic effects on signal fromnearby protons
Hemorrhagic strokeMRI
Natural history of hemoglobin in clot
oxyhemoglobin
deoxyhemoglobin
methemoglobin
Each molecule acts differently at MRI.
MRI in acute ΔMS
Standard T1 and T2 weighted images areinsensitive for small acute hemorrhage
Need CT first
Diffusion weighted images are highlysensitive for acute ischemia
Area of acute infarction visible within 30minutes of onset of ischemia
Subacute subdural hematomas
CT
MRI T1
MRI T2
Chronic subdural “hygroma” looks like fluid in all sequences
Subacute hematoma isodense on CT, bright on all MRI images
Take home messages:
Bleed or not?
CT for initial evaluation of acute ΔMS
MR more rapidly positive for acute ischemia
DWI positive within 20 minutes.
But: early identification of presence and sizeof infarct not usually necessary.
Only if thrombolysis is being considered
Take home messages:
Old or new stroke?
CT: look for water density and dilatation ofunderlying ventricle = old stroke.
MRI: water signal on T1 and T2 and low signal onDWI = old stroke
Cause of bleed?
Know typical locations of hypertensivehemorrhages:
Basal ganglia, cerebellum, pons
Review Questions
Concerning acute stroke: (T or F)
Patients are candidates for tPA thrombolysisup to 24 hours after onset of symptoms.
MRI is the modality of choice for initialevaluation of acute stroke symptoms.
Diffusion weighted imaging shows acuteinfarction earlier than any other modality.
50% are due to acute hemorrhage.
Hypertensive hemorrhage iscommon in all but:
Basal ganglia
Temporal lobe
Cerebellum
Brainstem
Intravenous contrast: all are trueexcept:
Contrast enhanced CT is not generally usefulin early stroke diagnosis
Persistence of contrast enhancement after 6-8weeks suggests underlying tumor.
Contrast enhanced MRI is more useful thanenhanced CT in early stroke.
Perfusion CT may help diagnose major strokeas rapidly as MRI
Additional reading
Beauchamp N et al. Imaging of acute cerebralischemia. Radiology:1999;212:307-324
Von Kummer R et al. Acute stroke: usefulness of earlyCT findings before thrombolytic therapy Radiology1997; 205: 327-333.
Hoeffner EG et al. Cerebral Perfusion CT: Techniqueand Clinical Applications Radiology 2004 231: 632-644
Provenzale JP et al. Assessment of the Patient withHyperacute Stroke: Imaging and Therapy Radiology2003;229:347-359.
The End
Use the back button on the browser to exit the program